Description of Disorder:
Duchenne muscular dystrophy (DMD) is a genetic disorder characterized by progressive muscle degeneration and weakness. This disorder first begins to affect the muscles of the hips, pelvic area, thighs and shoulders. Later the skeletal (voluntary) muscles in the arms, legs and trunk are also affected. The calves often are enlarged. By the early teens, the heart and respiratory muscles also are affected.
Cause of the disorder:
Those who inherit DMD have a defective gene related to a muscular protein called dystrophin. This protein keeps muscle cells intact. Its absence causes rapid muscular deterioration as a child with DMD grows. DMD is an X-linked recessive inheritance disorder. It is passed on by the mother.
Testing:
Genetic testing before conception can determine whether a couple has an increased risk of having children with DMD. Since this mutation isn’t in the mother’s blood cells, it’s impossible to detect by standard carrier testing. Prenatal testing is available for carriers. There are two main ways of performing a prenatal diagnosis. One is chorionic villus sampling, which involves removing tissue from the placenta for analysis. The other method is amniocentesis. A needle is inserted into your abdomen so that a sample of the amniotic fluid that surrounds the fetus in the womb can be taken.
Symptoms:
Symptoms include trouble walking, damage to the heart and lungs, scoliosis, tight muscles in his legs (contractures), headaches, problems with learning and memory, shortness of breath, sleepiness, and trouble concentrating.
Medical assistance:
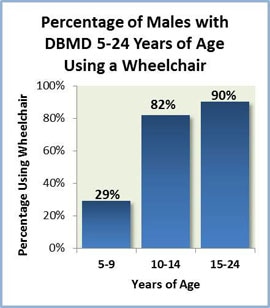
Braces, called orthoses, support the ankle and foot. These braces also may extend up over the knee. A standing walker or standing frame can assist people with DMD to stand. Eventually a wheelchair is needed in DMD, typically by about age 12. It is recommended that people with DMD have a complete cardiac evaluation by a specialist beginning in early childhood and again at least every other year until age 10. A range of motion exercises performed on a regular schedule can help the muscles from deteriorating. Until recently people with DMD usually did not survive much beyond their teen years. Due to the medical advances people surviving up until their 30s is much more common.
Reproduction:
A person with DMD can have children. Although if a male with DMD were to have children, all of his daughters would be carriers and none of his sons would be affected.
Treatments and Cures:
There is no known cure for Duchenne muscular dystrophy. Treatment can be used to control symptoms to improve quality of life. Steroid drugs can slow the loss of muscle strength. Other treatments include amino acids, carnitine, coenzyme Q10, creatine, fish oil, green tea extracts, vitamin E, assisted ventilation, and other drugs to help heart function.
Research:
In DMD, the muscle is missing a protein called dystrophin. Eventually the body can’t keep up with repair, which leads to muscle loss and weakness. Scientists therefore are working hard on the development of a number of therapies that could replace dystrophin, protect the muscle from injury and/or promote muscle repair and regrowth. Today there are many clinical trials currently being conducted.
Information:
Two websites you go to for more information are the Muscular Dystrophy Association and DMD Connecting Healthcare.
https://www.mda.org/
http://www.dmdconnects.com/
One organization for this disease is the Duchenne Foundation.
https://www.cureduchenne.org/
https://www.mda.org/
http://www.dmdconnects.com/
One organization for this disease is the Duchenne Foundation.
https://www.cureduchenne.org/
Interesting facts:
Since DMD is an x-linked genetic disease, males who inherit the mutation get the disease because they have no second dystrophin gene to make up for the faulty one. When a girl inherits a flawed dystrophin gene from one parent, she usually also gets a healthy dystrophin gene from her other parent, giving her enough of the protein to protect her from the disease. Usually girls don’t experience the full effects of DMD the way boys do, although they still have symptoms of muscle weakness.

|
|

|

|
Citations:
https://www.mda.org/disease/duchenne-muscular-dystrophy
https://medlineplus.gov/ency/article/000705.htm
http://www.webmd.com/children/duchenne-muscular-dystrophy
https://www.genome.gov/19518854/
http://www.healthline.com/health/duchenne-muscular-dystrophy
https://rarediseases.info.nih.gov/diseases/6291/duchenne-muscular-dystrophy
https://www.mda.org/disease/duchenne-muscular-dystrophy
https://medlineplus.gov/ency/article/000705.htm
http://www.webmd.com/children/duchenne-muscular-dystrophy
https://www.genome.gov/19518854/
http://www.healthline.com/health/duchenne-muscular-dystrophy
https://rarediseases.info.nih.gov/diseases/6291/duchenne-muscular-dystrophy
